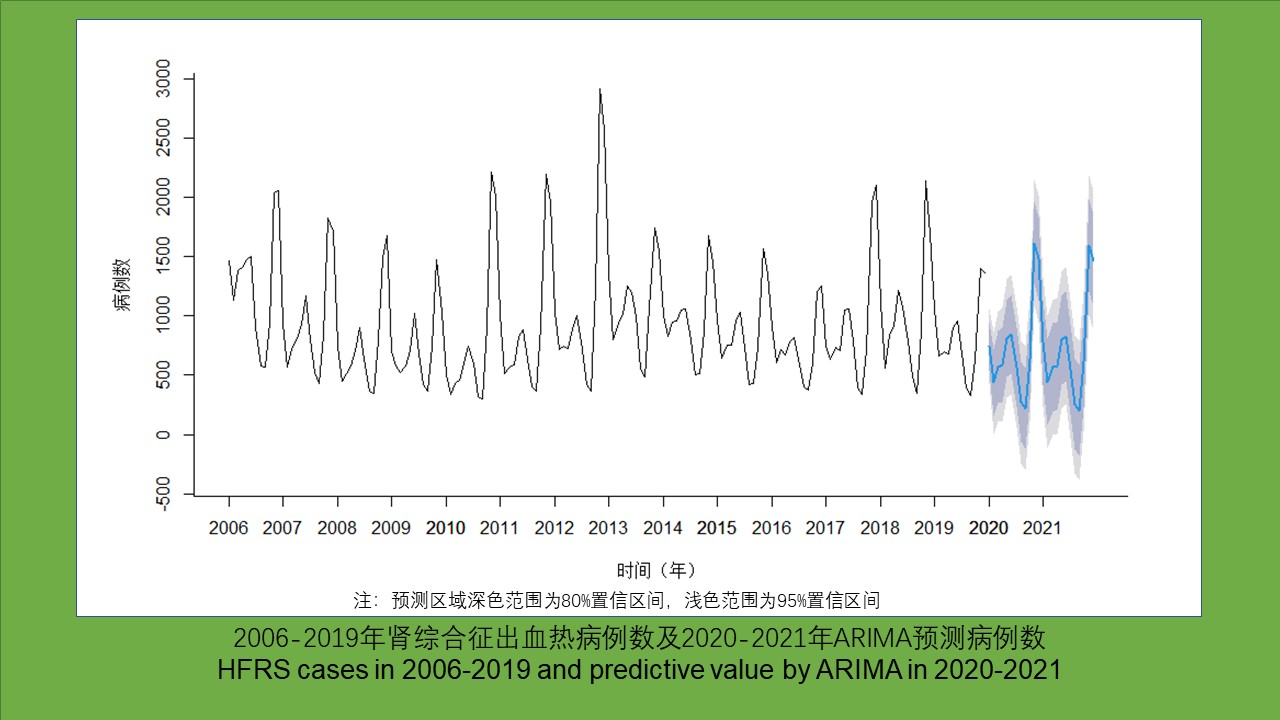
目的 分析2006-2021年我国肾综合征出血热(HFRS)的流行特征,探究新型冠状病毒肺炎(新冠肺炎)疫情流行期间我国采取的相关防疫政策是否对HFRS的流行情况产生影响,为后续制定相关政策提供科学依据。方法 应用描述性流行病学方法对我国2006-2021年HFRS流行特征进行统计分析,选取2006-2019年的HFRS病例数据建立自回归积分移动平均(ARIMA)模型,预测2020-2021年发病数,并对预测值与实际观测值进行比较。结果 2006-2021年间我国的HFRS病例数相对稳定,死亡病例显著减少。1年中有2个发病高峰,分别出现在5-6月和11月,具有明显的季节性。东北地区发病数降低,但在全国范围内流行范围扩大,且部分地区仍有暴发隐患。男性病例数明显高于女性,男性高发年龄段为35~49岁,女性为45~59岁,不同性别的发病年龄构成比差异有统计学意义(χ2=2 802.807,P<0.001)。农民仍是主要患病人群,占总病例数的半数以上。通过R 4.0.4软件拟合2006-2019年的HFRS病例数据建立季节性ARIMA模型为(2,0,2)(1,1,0)12,模型拟合效果好。2020-2021年HFRS病例实际观测值与预测值接近,在预测值95%置信区间内。结论 我国HFRS总体趋势较为平稳,仍是我国的重要公共卫生问题之一,需加强监测,实施更为精准的防控措施。2020-2021年间我国的新冠肺炎疫情防控措施对HFRS的流行情况未产生显著影响。
Objective To analyze the epidemiological characteristics of hemorrhagic fever with renal syndrome (HFRS) in China from 2006 to 2021, to investigate the influence of non-pharmaceutical intervention against coronavirus disease 2019 (COVID-19) on HFRS prevalence, and to provide a scientific basis for the subsequent formulation of relevant policies. Methods Descriptive epidemiological methods were utilized to statistically analyze the epidemiological characteristics of HFRS in China from 2006 to 2021. The data of HFRS cases from 2006 to 2019 were used to establish an autoregressive integrated moving average (ARIMA) model to predict the number of HFRS cases in 2020-2021, and the predicted values were compared with the actual observed values. Results The number of HFRS cases in China was relatively stable in 2006-2021, and the number of deaths were significantly reduced. HFRS had obvious seasonality, with two peaks of incidence in a year, i.e., May-June and November. The number of cases in northeast China decreased, but the affected areas in the whole country expanded, and some areas were still at risk of outbreak. The number of male cases was significantly higher than that of female cases. The peak age group of onset was 35-49 years for males and 45-59 years for females, and there was a significant difference in the age composition between males and females (χ2=2 802.807, P<0.001). Farmers were the main affected population, accounting for more than half of the total cases. The seasonal ARIMA model was established by fitting the data of HFRS cases from 2006 to 2019 with R 4.0.4 software, which was (2,0,2)(1,1,0)12 and was well fitted. The actual observed value of HFRS cases in 2020-2021 was close to the predicted value, within its 95% confidence interval. Conclusion HFRS is an important public health problem in China and the overall trend of its prevalence is relatively stable. It is necessary to strengthen the surveillance and implement more accurate prevention and control measures. The measures for COVID-19 prevention and control in China have no significant impact on the prevalence of HFRS during 2020-2021.
[1] Zhang YZ, Zou Y, Fu ZF, et al. Hantavirus infections in humans and animals, China[J]. Emerg Infect Dis, 2010, 16(8):1195-1203. DOI:10.3201/eid1608.090470.
[2] Cosgriff TM. Hemorrhagic fever with renal syndrome:Four decades of research[J]. Ann Intern Med, 1989, 110(4):313-316. DOI:10.7326/0003-4819-110-4-313.
[3] 刘起勇. 2005-2020年我国媒介生物传染病报告病例:流行趋势、防控挑战及应对策略[J]. 中国媒介生物学及控制杂志, 2022, 33(1):1-7. DOI:10.11853/j.issn.1003.8280.2022.01.001. Liu QY. Reported cases of vector-borne diseases in China, 2005-2020:Epidemic trend, challenges in prevention and control, and related coping strategies[J]. Chin J Vect Biol Control, 2022, 33(1):1-7. DOI:10.11853/j.issn.1003.8280.2022.01.001.(in Chinese)
[4] Xiao JP, Dai JY, Hu JX, et al. Co-benefits of nonpharmaceutical intervention against COVID-19 on infectious diseases in China:A large population-based observational study[J]. Lancet Reg Health West Pac, 2021, 17:100282. DOI:10.1016/j.lanwpc. 2021.100282.
[5] Geng MJ, Zhang HY, Yu LJ, et al. Changes in notifiable infectious disease incidence in China during the COVID-19 pandemic[J]. Nat Commun, 2021, 12(1):6923. DOI:10.1038/s41467-021-27292-7.
[6] Das RC. Forecasting incidences of COVID-19 using Box-Jenkins method for the period July 12-Septembert 11, 2020:A study on highly affected countries[J]. Chaos Solitons Fractals, 2020, 140:110248. DOI:10.1016/j.chaos.2020.110248.
[7] Toğa G, Atalay B, Toksari MD. COVID-19 prevalence forecasting using autoregressive integrated moving average (ARIMA) and Artificial Neural Networks (ANN):Case of Turkey[J]. J Infect Public Health, 2021, 14(7):811-816. DOI:10.1016/j.jiph. 2021.04.015.
[8] Kabacoff RI. R语言实战(第2版)[M]. 王小宁, 刘撷芯, 黄俊文, 等, 译. 北京:人民邮电出版社, 2016:333-339. Kabacoff RI. R in action:Data analysis and graphics with R (2nd ed)[M]. Wang XN, Liu XX, Huang JW, et al, Translation. Beijing:Posts & Telecon Press, 2016:333-339.(in Chinese)
[9] 刘怀文. 我国流行性出血热的概况[J]. 医药产业资讯, 2006, 3(21):121-123. DOI:10.3969/j.issn.1673-7210.2006.21.098. Liu HW. General situation of epidemic hemorrhagic fever in China[J]. Med Ind Inf, 2006, 3(21):121-123. DOI:10.3969/j.issn.1673-7210.2006.21.098.(in Chinese)
[10] 杨其松. 2010-2017年宜春市肾综合征出血热时空分布特征与经济负担研究[D]. 南昌:南昌大学, 2019. Yang QS. Study on spatio-temporal distribution and economic burden of hemorrhagic fever with renal syndrome in Yichun city from 2010 to 2017[D]. Nanchang:Nanchang University, 2019. (in Chinese)
[11] Koutsakos M, Wheatley AK, Laurie K, et al. Influenza lineage extinction during the COVID-19 pandemic?[J]. Nat Rev Microbiol, 2021, 19(12):741-742. DOI:10.1038/s41579-021-00642-4.
[12] Hao XJ, Cheng SS, Wu DG, et al. Reconstruction of the full transmission dynamics of COVID-19 in Wuhan[J]. Nature, 2020, 584(7821):420-424. DOI:10.1038/s41586-020-2554-8.
[13] 宋干. 新中国流行性出血热防治研究的主要成就[J]. 中华流行病学杂志, 2000, 21(5):378-382. DOI:10.3760/j.issn:0254-6450.2000.05.019. Song G. The main achievements of epidemic hemorrhagic fever prevention and control in China[J]. Chin J Epidemiol, 2000, 21(5):378-382. DOI:10.3760/j.issn:0254-6450.2000.05.019.(in Chinese)
[14] 吴光华. 近年中国肾综合征出血热流行病学研究进展[J]. 中华流行病学杂志, 2003, 42(5):413-415. DOI:10.3760/j.issn:0254-6450.2003.05.024. Wu GH. Advances in epidemiology of hemorrhagic fever with renal syndrome in China[J]. Chin J Epidemiol, 2003, 42(5):413-415. DOI:10.3760/j.issn:0254-6450.2003.05.024.(in Chinese)

